
WHO has just released the latest update on global causes of death for children under age 5 for years 2000-2017. These are available for download on the WHO website at https://www.who.int/healthinfo/global_burden_disease/estimates/en/index2.html and also in the Global Health Observatory at www.who.int/gho. A collaborating group of academic researchers led by Professor Bob Black from Johns Hopkins University carried out data analysis and modelling in collaboration with a number of WHO technical departments and myself.
Despite remarkable progress in the improvement of child survival globally, with a reduction in the annual number of child deaths from 10 million in 2000 to 5.4 million in 2017, this level of progress will need to accelerate to achieve the Sustainable Development Goal for child mortality in 2030. There remain many preventable child deaths in developing countries. The causes of the 5.4 million deaths of children under 5 are summarized in the following pie chart.

Global distribution of causes of child death under age 5, 2017
Almost half of deaths under 5 are now in the neonatal period (the first four weeks of life) where the causes of death are shaded yellow above and led by prematurity and birth asphyxia or trauma. In the period 1-11 months the leading cause of death is acute respiratory infection (ARI) which is mostly pneumonia, followed by diarrheal diseases and injuries.
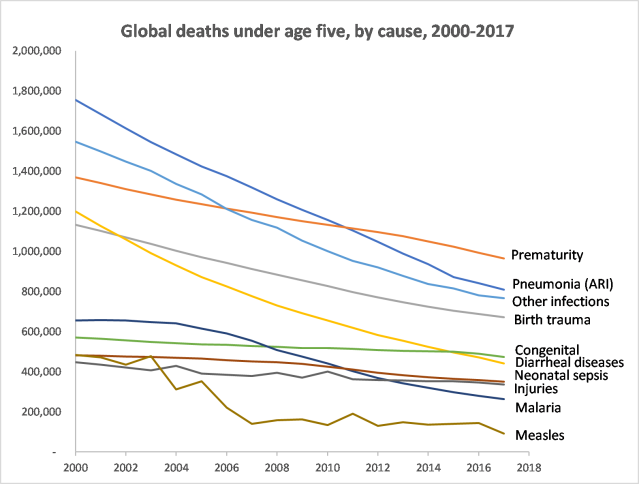
Reductions in mortality rates for pneumonia, diarrhoea, neonatal intrapartum-related events, malaria, and measles were responsible for 65% of the total reduction of under 5 deaths, pr just under 3 million of the 4.6 million deaths per year averted between 2000 and 2017 (see Figure below). Most of these causes relate mainly to the period 1-59 months after the neonatal period. The faster decline in these “post-neonatal” causes over the last 15 years has resulted in preterm birth complications now being the leading cause of under 5 deaths in 2017.
I first got involved in the analysis of global child causes of death under age 5 in 2001, when the WHO Child Health Epidemiology Reference Group (CHERG) was formed. Members of the CHERG collaborated with WHO staff to publish global, regional and country-level estimates of neonatal and 1-59 month deaths, which were updated a number of times over subsequent years with continuing improvements in modelling and results. From 2012 onwards, the CHERG and WHO moved to the regular publication of time series of child causes of deaths from 2000 to latest year. About five years ago, former CHERG members received funding from the Bill and Melinda Gates Foundation to continue collaborative work with WHO as the Maternal and Child Epidemiology Estimates Group (MCEE).
The methods developed by CHERG and MCEE involve the simultaneous estimation of a set of linked regression models for 15 causes of child deaths, in such a way that the estimated cause fractions are constrained to sum to 1. These fractions are then applied to the all-cause “envelopes” of child deaths to generate numbers of deaths by cause over time.
For around 76 countries with high-quality vital registration (VR) data, cause distributions are estimated directly from the death registration data. For another 37 countries with low child mortality, cause of death distributions are predicted from a regression fit to data from countries with high-quality VR data. For higher mortality countries without high-quality VR data, cause of death distributions are predicted from a regression fit to data assembled from studies of causes of death in high-mortality countries, which typically rely on verbal autopsy. These approaches are augmented by WHO and UN program estimates for certain diseases, such as HIV and measles.
Deaths due to malaria are estimated from the high-mortality regression model for African countries in the endemic malaria regions, and for other countries in Africa and the rest of the world from health system and survey data. MCEE works closely with the WHO Global Malaria Program to prepare the malaria mortality estimates for children under 5 and the results are also reported in the World Malaria Report 2018 (https://www.who.int/malaria/publications/world-malaria-report-2018/en/). For countries in the African Region where malaria comprises 5% or more of all deaths in children under 5, child malaria deaths were estimated using a verbal autopsy multi-cause model. This model includes malaria parasite prevalence (PfPR) as a covariate at study level for the data observations and uses national average PfPR for the country-level output estimates. The estimates of PfPR are made by the Malaria Atlas Project at Oxford University (https://map.ox.ac.uk/) using a geostatistical model that incorporates changes in coverage of malaria interventions (insecticide treated bed nets, indoor residual spraying, antimalarial treatment) over time to produce a risk map of parasite prevalence for each year

Pingback: State-level trends and levels of child mortality in India 2000-2015 | Colin Mathers